
A sideways curvature of the spine characterizes scoliosis, which is surprisingly common. Most people with minor scoliosis go through life and may never even know they have the condition. However, if scoliosis progresses to a significant C- or S-curve of the spine, it becomes a problem.
Types of Scoliosis
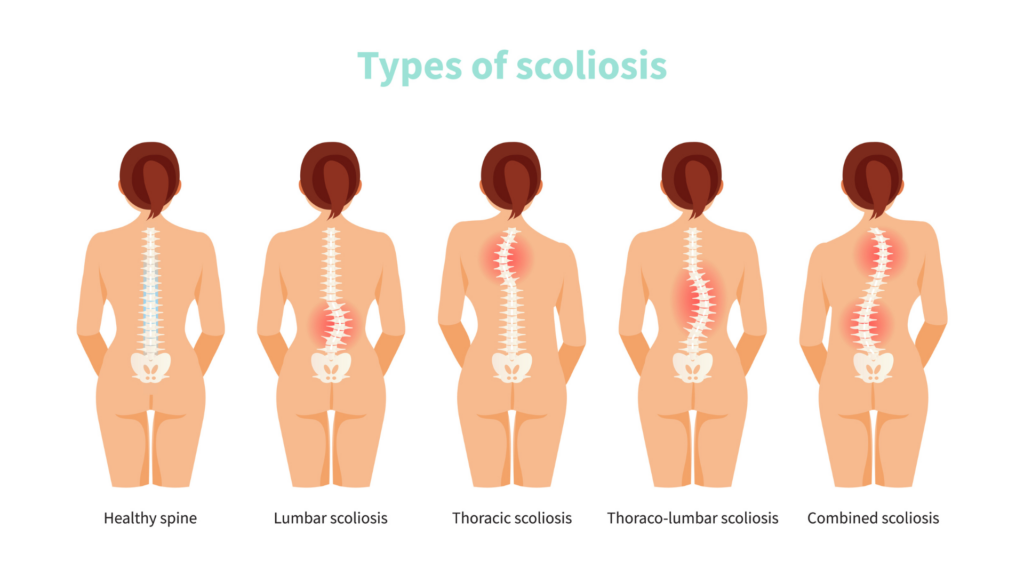
Contemporary medicine defines two major types of scoliosis: Degenerative, due to structural changes in vertebrae, discs, and the ligaments that hold them together, generally seen in people beyond 50, and Adolescent Idiopathic, which literally means “without any (known) cause.” Less commonly, scoliosis may be due to neurological diseases such as cerebral palsy, congenital muscular weakness, and system-wide problems such as osteogenesis imperfecta, in which the bones themselves are soft and readily deformable.
The architect Buckminster Fuller’s concept of a tensegrity structure: a structure held up by tension between its parts, is useful in understanding scoliosis. A teepee or wigwam is a tensegrity structure since each of the poles that hold up the teepee would crash to the ground if it were not opposed by another pole leaning in the opposite direction. Another example is a radio antenna, such as you might see on a drive through the country. It is held up, paradoxically, by cables pulling downward. Still, since they do so symmetrically – the pressure pulling to the right is equal to the pull from the cables on the left, the antenna straight and vertical.
The human spine is another tensegrity structure, but a more complicated one. True, it is held up by muscles symmetrically exerting force from the right, left, and front to back. Still, unlike the architectural examples, the spine is articulated and capable of movement in all three planes: front-to-back, side-to-side, and rotation. Just about every member of the phylum Chordata, except possibly the turtle, has such a spine; none other has lost the ability to bend and twist. Survival appears to require a backbone with two core abilities: being stiff enough to hold us up but sufficiently flexible to enable motion in all three of those planes, usually in all three of them at once. In these respects, the spine departs from any architectural realm, since it is part of living, moving, and dynamic creatures.
How Yoga Can Help Reverse Scoliosis

So unlike the work of architects, mere support is only half of the spine’s function. Still, the forces exerted by muscles are responsible for their erectness and motion. We have found that understanding the muscles that hold and move the spine yields a valuable way to reverse both common types of scoliosis. Yoga turns out to be a simple and effective means to apply it. We have also been able to help some people with osteogenesis imperfecta. The key is understanding the conditions underlying scoliosis.
Suppose the muscles on the right are stronger and are pulling the spine in that direction. In that case, the spine will curve toward the right, becoming convex to the left. What often happens next is that the left-sided ribs begin to splay out like the spokes of a wheel, stretching the skin and muscles of the back on that side and then migrating into the space created by their increased separation. This leads to a bulge on the convex side, which for centuries led many people to believe that the convex side was stronger. Nothing could be further from the truth. Actually, that bulge is hollow, and the strong side is the indented side, compressed by more powerful muscles shortened because they are contracting.
Strengthening the quadratus lumborum and paraspinal muscles of the convex side works to equalize and balance the muscular tensions that produce and sustain degenerative and adolescent idiopathic scoliosis. A small variation to the Iyengar version of the side-plank, Vasisthasana, has proven to be a reliable way to accomplish this in our studies so far. We took X-rays of patients’ spines before and after months of daily practice of the pose, done once daily and held for as long a period of time as possible, for 3 -22 months. Just using a slightly modified Vasisthasana reduced degenerative scoliotic curves by an average of 34% and adolescent idiopathic curves by an average of 49.6% in a mean of 6.8 months of daily practice.
Scoliosis is an asymmetrical condition and appears to require an asymmetrical remedy. We have recommended only practicing it with the lumbar curve’s convex (weaker) side facing downward.
Some scoliotic curves are a simple “C,” generally in the lumbar or lumbar and thoracic spine. Others are “S” or inverted “S” in their shape, and a few are triple or even quadruple curves. In our first study of 25 patients, we concentrated on the lowest curve, only using Vasisthasana and only with the convex side downward. However, we found that the upper curves also got smaller, but not as quickly and not as much. Some researchers believe that the upper curves can be compensatory, which would explain this effect. Nevertheless, We are working with other postures and having somewhat better results with the upper curves at this point. The more complex curves require individual analysis.
We have done MRI studies with Vasisthasana. It appears quite useful in treating spondylolisthesis and herniated lumbar discs and improving posture, balance, and, not surprisingly, core strength. These applications generally require doing the pose on both sides, but there are special adaptations here too.
 Dr. Loren Fishman is a medical doctor and lifelong student of yoga, including extensive studies with B.K.S. Iyengar in India. As a practicing MD, Dr. Fishman has become known as a leading pioneer in the integration of yoga in rehabilitative medicine. Dr. Fishman is the author of several books in addition to the books co-authored with Ellen Saltonstall.
Dr. Loren Fishman is a medical doctor and lifelong student of yoga, including extensive studies with B.K.S. Iyengar in India. As a practicing MD, Dr. Fishman has become known as a leading pioneer in the integration of yoga in rehabilitative medicine. Dr. Fishman is the author of several books in addition to the books co-authored with Ellen Saltonstall.
